In this short interview, author Iain Crossingham, Consultant Intensivist and Respiratory Physician, tells us more about this review and the treatment of airways diseases.
Tell us about this Cochrane Review
This is an interesting time for the treatment of airways diseases. Traditionally we've thought of these as coming under two main headings, asthma and chronic obstructive pulmonary disease (COPD), plus a handful of other rarer conditions such as bronchiectasis. Characteristically asthma caused variation in lung function tests such as peak flow or FEV1, either over time or with medication whereas COPD is defined by lung function that didn't improve ("fixed airflow obstruction"). Basing diagnosis on one dimension of the disease process (how quickly someone come blow air out of their lungs) obviously misses many other aspects of these conditions including the symptoms that impact people on a day to day basis.
In the clinic, we come across many different disease traits, for example
- Wheeze/airflow obstruction
- Cough, either daytime or disturbing sleep overnight
- Sputum production, either intermittent or continuous
- Frequent "exacerbations" or flare ups of symptoms
- Structural changes in the lungs seen on CT scans
- Persistent breathlessness and exercise intolerance
- Association of symptoms with exposures at work or elsewhere
Why was it important to do this systematic review?
People may experience any of these and other traits regardless of whether their "official" label is asthma or COPD (or something else). Identifying the traits present in a particular individual at a particular time is what the pragmatic physician does to help agree a personalised treatment plan with an individual patient. This presents a problem for someone trying to be "evidence based" as trials have mostly lumped participants into broad but heterogenous groups based on diagnostic labels.
Why is this review important for people living with COPD and the clinicians treating them?
We've tried in this review to look at what are considered "asthma" treatments (anti IL5 drugs) in individuals with COPD who nonetheless may have traits that might respond to these drugs. We'd planned specific subgroup analyses looking at those with raised levels of particular biomarkers such as peripheral blood eosinophil counts that might define certain traits. The included trials were somewhat of a disappointment, mostly taking all comers rather than targeting groups who theoretically might respond. These were "lumper" trials, looking for(and on the whole failing to find) a modest benefit in a whole population. As you might have gathered, I think we need to split these groups down and personalise our treatments.
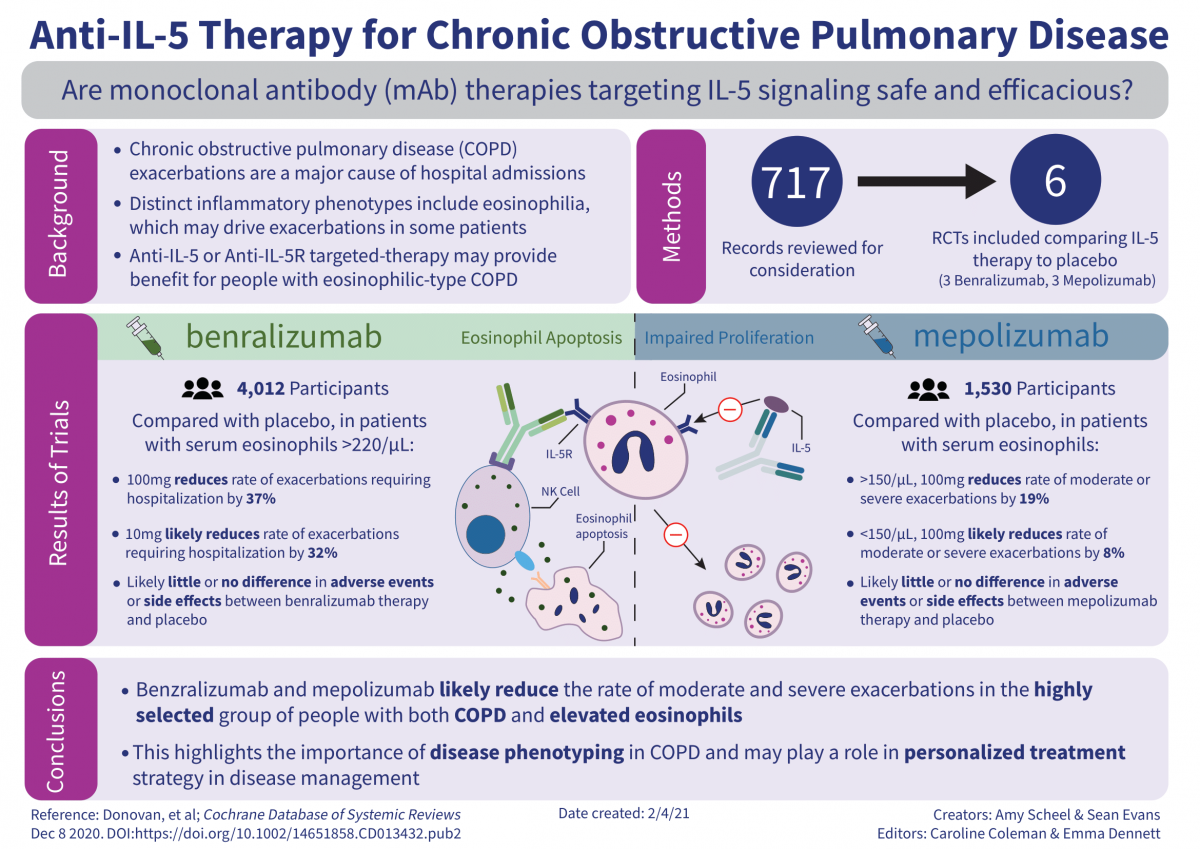
Learn more about this visual abstract
View PDF of visual abstract
What can people living with COPD and clinicians treating them take from this evidence?
Should people living with COPD or their clinicians be racing to start anti-IL5 drugs? No. However this is hopefully just a start. In the future, I'd like to see a person with an airways disease (be it labelled asthma or COPD) be able to choose the evidence based treatments that work for their particular set of problems and avoid the therapies that aren't relevant to their manifesting disease traits. There is clearly a challenge to us systematic reviewers. How do we collect evidence when the diagnostic labels used in trials don't capture the breadth of the experience of those living with the conditions?




